Quick info

Methamphetamine (N-methylamphetamine) is a synthetic amphetamine derivative. Like amphetamine , methamphetamine triggers the release of dopamine and norepinephrine in the brain, thereby producing euphoria and increasing energy. Since methamphetamine reaches the brain more quickly than amphetamine and its stimulating effect is stronger and longer-lasting, it produces a more intense and longer-lasting high (kick) and therefore has a higher potential for addiction than amphetamine.
Norepinephrine and dopamine are released simultaneously; pronounced subjective performance enhancement, increased self-esteem, euphoria, disinhibition and increase in desire; methamphetamine is therefore also used as a sex drug. Increase in body temperature, accelerated pulse and respiration, and increased blood pressure. Hunger, the need for sleep, and pain are suppressed. Increased willingness to take risks, increased aggressiveness and readiness to use violence, extreme nervousness, and an increased urge to talk (babble flush) are further characteristics of its effects. Methamphetamine is broken down only slowly in the body.
Onset of effect
Snorted after approx. 10-20 minutes, swallowed after 30-120 minutes, smoked and injected within a few seconds
Duration of action
Depending on the form of application 3-12 hours. In high doses, the effect can last longer than 24 hours
Aftereffects
up to 70 hours
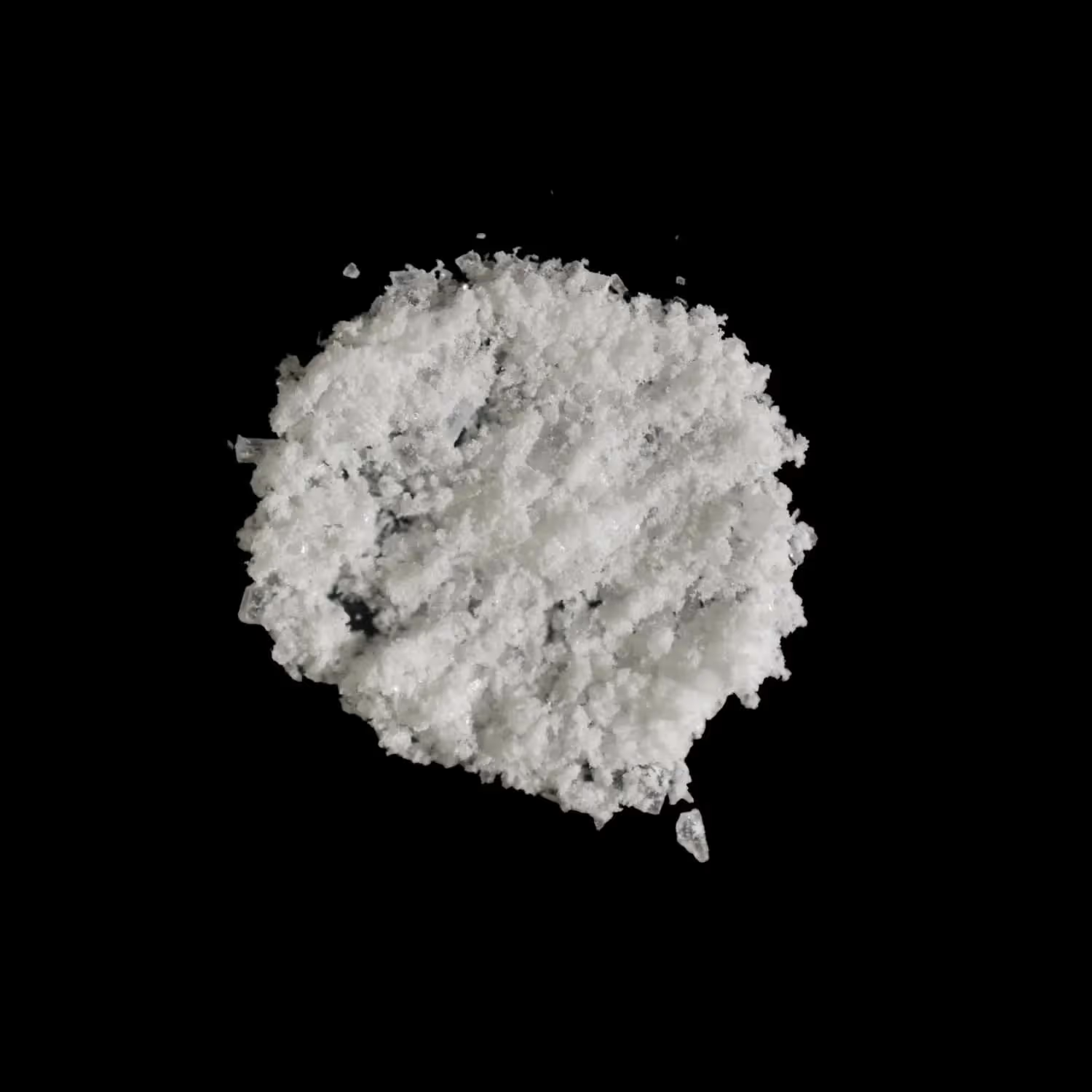
Appearances
Pills (Yaba, Thaipille, Pervitin®) or crystalline powder (Crystal, Ice, Pico)
Forms of consumption
Methamphetamine is swallowed, snorted, smoked, injected (slamming) or administered rectally
Swallowed:
Light: 5 - 10 mg
Medium: 10 - 25 mg
Strong: 25 - 50 mg
Very strong: +50 mg
Intravenous (slamming):
Light: 5 - 10 mg
Average: 10–20 mg
Strong: 20–30 mg
Very Strong: +30 mg
Snuffed:
Light: 5 - 10 mg
Medium: 10 - 30 mg
Strong: 30–50 mg
Very Strong: +50 mg
Smoked:
Light: 5 - 10 mg
Medium: 10 - 25 mg
Strong: 25 - 50 mg
Very strong: + 50 mg
If in doubt, proceed cautiously with the dosage and start with a low dose to avoid overdoses and health risks. The dosage instructions are based on 100% pure content.
Short-term side effects include tense jaw muscles, dry mouth, increased body temperature, marked dehydration and increased heart rate, as well as increased blood pressure and tremors all over the body, irritability and aggressive to violent behavior (especially in combination with alcohol and in high doses). Individuals with methamphetamine overdoses usually experience psychiatric symptoms such as agitation, suicidal ideation, or psychotic reactions. Deaths associated with methamphetamine overdoses are usually due to pulmonary edema, cerebral hemorrhage, cardiac arrhythmias, acute heart failure, or high fever.
Long-term risks
Methamphetamine is a highly depleting substance with a very high dependency potential with psychological and physical withdrawal symptoms. Pronounced downs, aggression, depression and the desire to use again (craving) characterize the period of regular use. This can lead to constant restlessness, sleep and circulatory disorders, paranoia and even amphetamine psychosis. Suicidal thoughts also occur frequently. Weight loss, skin inflammation ("speed pimples"), tooth loss, kidney and lung damage, stomach problems and epileptic seizures are also possible. In women, the menstrual cycle can be disrupted. Sniffing damages the nasal mucous membranes and nasal septum, swallowing damages the stomach mucous membranes; smoking damages the lungs and increases the risk of cancer. Chronic consumption promotes cerebral hemorrhages and strokes with sudden paralysis and damages the heart.
It is believed that chronic use of methamphetamine can irreversibly alter or damage the brain, associated with impairments in intellectual performance. Chronic methamphetamine users have a significantly increased risk of Parkinson's disease.
If you or someone else needs urgent help after taking drugs or alcohol, call an ambulance on 144. Tell the emergency responders everything you know.
It could save lives.